
Research Article | DOI: https://doi.org/10.31579/2578-8868/113
Neurosurgeon in Mexico City, Mexico
*Corresponding Author: Carlos Francisco Gutierrez Partida, Neurosurgeon in Mexico City, Mexico
Citation: Gutierrez Partida CF., Javier Q. Olvera., Velazquez Aleman AP., Ramirez leon. JF, Carlolina R Martinez. (2020) Minimally Invasive Transforaminal lumbar Interbody Fusion: when does the Learning Curve Begin?. J. Neuroscience and Neurological Surgery. 6(2); DOI:10.31579/2578-8868/113
Copyright: © 2020 Carlos Francisco Gutierrez Partida, This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Received: 19 December 2019 | Accepted: 22 January 2020 | Published: 03 February 2020
Keywords: minimally invasive; transforaminal lumbar
A recent studies have reported the learning curve in minimally invasive transforaminal lumbar interbody fusion (MI-TLIF). Over the last two decades there has been a growing interest for the treatment of spinal disorders performed through the use of minimally invasive surgical procedures. The studies are based on clinical result such as blood loss, surgical time, or high rate of perioperative complications but none have studied the origin of these results. This study proposes a systematic learning skills method and a different perspective to evaluate the MI-TLIF learning curve.
Over the last two decades there has been a growing interest for the treatment of spinal disorders performed through the use of minimally invasive surgical procedures. [1,2] Actually, several manuscripts reported successful results associated with MI-TLIF. Also, differents authors evidenced that MI-TLIF procedures provide benefits regarding estimated blood loss, postoperative pain intensity, and length of hospital stay. [3,4,5] Some disadvantages of this technique are: the difficulty associated with working through a narrow surgical corridor that limits visualization of important anatomical landmarks and its steep learning curve. [6,7] A few articles report the existence of a learning curve applied to MI-TLIF, taking into account perioperative and postoperative data. [1,6,7,8] Furthermore, another studies refer that the rate of complications is the best indicator reflecting the experience of a spine surgeon; same studies that recommend to be cautious during initial MI-TLIF procedures to avoid complications associated to the learning effect. [6,7,8,9] However, no study answers the following questions: When does the learning curve originate? Does the curve only reflect the results of performing the technique repeatedly? Based on these concepts, we decided to evaluate the learning process of MI-TLIF technique by first using a systematic learning skills method and subsequently evaluating how that process determined the results of the learning curve in a minimally invasive spine fellow throughout his transition into becoming a minimally invasive spine surgeon.
Materials and Methods
Systematic learning skills method
This method proposes to organize the learning process of a complex minimally invasive spine technique, dividing it into tasks or steps that result in the complete implementation of such. These steps should be gradually learned in able to perform the complete technique fluidly. Surgical skills were evaluated using the OSATS global rating scale. [10] Evaluations were carried out by the surgeons who participated in the procedure. The first assessment of these tasks was developed at 18 months of such training. Subsequently, the last 6 months were also evaluated. The tasks that the MI-TLIF technique were divided into represent the key steps that compose it. These tasks were: [1] Patient placement, [2] Fluoroscopic planning, [3] Incision, [4] Tubular retractor docking, [5] Facetectomy with high-speed drill, [6] Microdiscectomy, (7) Endplate preparation, [8] Bone graft placement, [9] Cage introduction, [10] Pedicle screw placement. It is important to mention that the training period duration of the Minimally Invasive Spine Surgery (MISS)-fellow, who was assessed, lasted 2 years. During this period the MISS-fellow participated in courses, cadaver workshops, and academic sessions that strengthen the theoretical knowledge of the MI-TLIF technique.
The Learning Curve
The approval of local ethics committee was obtained. We retrospectively reviewed clinical records of all patients who underwent MI-TLIF procedures performed by the index author from February 2012 to March 2015. All patients included in the learning curve were operated after concluding the surgeon’s training period, therefore posterior to finalizing the systematic learning skills method described. Inclusion criteria were: adult patients, both genders, with degenerative lumbar spine disease, and without clinical improvement to conservative treatment for a least six months’ period prior to MI-TLIF. In addition, we excluded patients in which revision surgery was performed. With these selection criteria we included fifty-four patients as a discretionary sampling.
Measured parameters
Perioperative parameters included: patient demographics, operative time, estimated blood loss, perioperative and posoperative complications, and length of hospital stay. Visual Analogue Scale (VAS) for back and leg pain, Oswestry Disability Index (ODI), and the 36-Item Short Form Health Survey (SF-36) were preoperatively assessed and at 5 and 12 months after surgery.
Surgical technique
The patient will be in prone position under general anesthesia, continuous neurophysiologic monitoring (a really important tool), and fluoroscopic image guidance with C-arm, surgical approach was performed on the most symptomatic side. Progressive tubular retractors were used. Minimally invasive surgical procedure was performed through a 16 mm diameter working cannula. Complete lateral facetectomy and discectomy were performed; the endplates were prepared and bone graft was delivered in the lumbar intersomatic space. A rectangular bullet-nose cage was inserted. Cannulated transpedicular screws were placed afterwards.
Statistical analysis
Descriptive statistics was performed using SPSS version 17.0 statistical software. The clinical records were sequentially ordered according to date of surgery. Surgical time was properly adjusted on patients undergoing a multilevel MI-TLIF procedure. [12] The learning curve based on surgical time was calculated by piecewise regression analysis using the mathematical algorithm described by Muggeo, [13] (SigmaPlot statistical software version 12.3).
Results
Systematic learning skills method
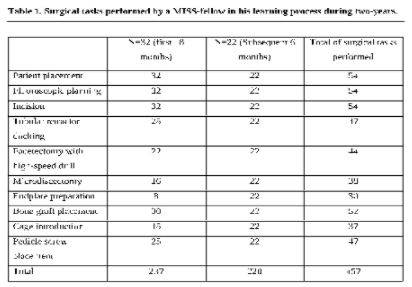
The surgical tasks performed by the MISS-fellow during his learning process of MI-TLIF technique, during the first 18 months, were a total of 237 tasks on 32 patients. During the last 6 months he performed 220 tasks on 22 patients.
Consequently, the surgeon acquired more experience as he performed more tasks throughout the learning process. The evaluation of surgical skills with OSATS global rating scale rated 27 points in the first 237 tasks and 30 points in the subsequent 220 tasks. This means that the fluidity of the procedure improved in terms of task execution during the last 6 months analyzed. Table 1
The learning curve
Piecewise regression analysis evidenced that according to operative time in MI-TLIF, there is a break point at the 16th patient. Figure 1 The moving range chart demonstrated longer surgical time in patients 9, 26, and 36 despite the average operating time.

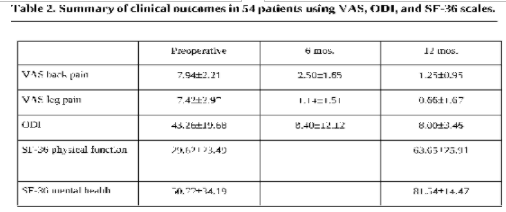
The Figure 2 of 54 patients evaluated from February 2012 to March 2015, 30 patients (55.5%) were female and 24 patients (44.4%) were male. Mean (SD) age of the patients was 68.917.18 years (range from 65-89 years). Two-level surgery was performed in 19 patients (35.18%) while 2 cases (3.7%) required a three-level fusion surgery. Mean (SD) operative time was 182.463.6 min (range 90-340 min) while the mean (SD) estimated blood loss was 43.834.1 mL (range 10-250 mL). The median hospital length stay was 3 days (IQR 2-10 days). VAS back and leg pain as well as ODI were assessed preoperatively and at the 6 and 12 month mark. SF-36 survey was evaluated preoperatively and at the final follow-up. Table 2 None of the cases required conversion to open surgery.
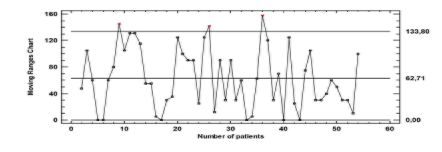
No perioperative complications occurred. The ability to treat conditions of the spine through the use of minimally invasive surgical techniques has gained interest amongst spine surgeons and their patients over the last two decades. [1,2] Web, et al assessed the arguments emitted by eighty-seven spine surgeons about limitations and disadvantages of MISS techniques and they concluded that there is a lack of effectiveness, technical difficulty, radiation exposure, and very few opportunities to learn these types of techniques; a fact that is more prominent in Latin American countries. [14] Specifically talking about MI-TLIF, the results of recent clinical studies and meta-analysis showed benefits regarding perioperative bleeding, postoperative pain, hospital length stays, infection rates, and overall costs. Other studies consider the rate of complications the best clinical indicator of the spine surgeon ́s experience and recommend to be cautious during the initial procedures to avoid potential complications related to the learning effect. [3,5,6,7,8,9] The learning curves in MI-TLIF published by authors like Nandyala, et al referred perioperative outcomes in sixty-five procedures of MI- TLIF and demonstrated longer surgical time, more blood loss, and increased anesthetic time in the first thirty-three cases. In addition, the frequency of complications and hospital length stay were similar to those operated by conventional open surgery. [15] Schizas, et al reported a learning curve in MI-TLIF that showed decreased surgical time after twelve patients were operated consecutively and also showed no increase in the frequency of complications associated to the learning effect. [8] Lee, et al reported a learning curve of MI-TLIF reached after 30 cases. They compared their first 30 cases with subsequent ones which had less operating time, estimated blood loss, and hospital length stay. [16] It is important to remember that the principle underlying the learning curve is well established: performing tasks in repetitive fashion reduces the time to complete them and increases the quality of those tasks. Therefore, the learning curve must be interpreted according to its specific context. In this study, a learning curve associated with surgical time was estimated in 54 patients who underwent MI-TLIF by a MISS-surgeon that completed his training period using a different learning process that, up until now, had not been described: the systematic learning skills method. The learning curve showed stabilization in surgical time after the 16th patient. Figure 1 piecewise regression analysis estimates the break point at the 16th patient.
A complications variable was not considered for the learning curve development because there were no complications reported in any of the 54 patients. This reinforces the fact that the learning method is crucial for good clinical results and that the surgical time depends on the clinical scenario characterized by performing the whole technique on real patients.
This demonstrates that the progressive acquisition of the surgical skills is needed to perform a fluid and safe MI-TLIF technique in a real clinical scenario. Applying the learning skills method when executing the technique ensures that the young MISS-Surgeon can avoid complications, and if any were to arise he would have the proper knowledge to approach them. Therefore, we think that the initial experience in MI-TLIF is acquired with the partial execution of numerous key tasks of the technique. The mastery of individual surgical tasks is verified by the fluency and ergonomics of movements, which leads to surgical proficiency throughout the whole procedure. Figure 3
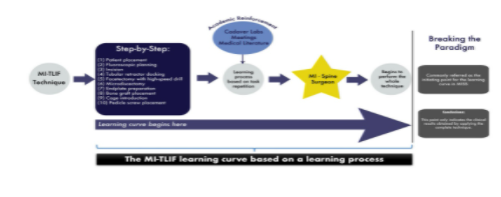
When does the learning curve originate? We consider that the learning curve in MI-TLIF starts with sequential training and knowledge of every step that conforms the whole technique, beginning with the surgeon’s training. The learning curve is also influenced by the number and repetition of surgical tasks performed in particular clinical scenarios (patient individual setting). We determined that the learning curve is influenced by the application of the totality of the technique in his surgical practice as a faculty surgeon. In addition, the whole process of experience is completed by the academic labor of the surgeon. This was the proposed method in this article. After this analysis, we establish that the learning curve should be understood as a process that leads to clinical results. Therefore, the clinical results obtained after preforming the whole technique do not represent the totality of the learning curve, they are just a part of it. This article tries to change the paradigm established by previous literature which states that the learning curve is limited to just the clinical outcomes and instead to consider it as a measurement of the learning skills obtained up until the point when the whole procedure can be accomplished.
This method could be implemented in the teaching and learning process for future MIS-Surgeon´s training applied in each and every other minimally invasive spine surgery technique.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
